Can you believe that one of humanity’s deadliest pathogens, which continues to challenge us every day, was once romanticised and associated with fragility and beauty?
In the 1800s, Tuberculosis (TB) was commonly known as consumption because it caused people to become progressively thinner and weaker. Long before scientists discovered the bacterium responsible for the disease, its victims were often described as possessing a strange and tragic beauty. Pale skin, rosy cheeks, and a slender frame, all hallmarks of advanced TB, became fashionable traits in parts of Europe, inspiring artists, writers, and even beauty trends. What people did not realise was that behind this romantic image lurked the deadly Mycobacterium tuberculosis.
The bacterium was discovered by Robert Koch in 1882. More than a century later, TB continues to infect millions of people every year, particularly in low- and middle-income countries such as India, with 2024 recording more than 3 Lakhs deaths due to TB. Adding to the challenge, Mycobacterium tuberculosis has evolved a formidable new weapon: resistance to antibiotics, the very drugs designed to kill it.
Meet the microbe
Mtb, short for Mycobacterium tuberculosis, is a remarkably resilient bacterium.
It is shaped like a tiny rod and is about 100 times thinner than a human hair. Unlike many bacteria, Mtb grows very slowly and is protected by a thick, waxy cell wall rich in mycolic acids. This unique outer coat acts like a suit of armour, helping the bacterium survive harsh conditions and making it more difficult for many antibiotics to penetrate and kill it.
The secret to TB’s success
The success of this pathogen lies not in its size or shape, but in its extraordinary ability to spread, persist, and hide.
Tuberculosis is an airborne disease that begins when a person inhales tiny droplets containing Mtb. The bacteria usually establish infection in the lungs, where they encounter the body’s first line of immune defence. Although the immune system is often able to control the infection, eliminating the bacterium completely is much more difficult.
What makes Mtb interesting is its ability to live silently in a human body for years without showing any signs of infection. In many infected individuals, the bacteria persist in a dormant state known as latent TB infection. During this phase, people do not feel sick and cannot spread the disease. However, if the immune system becomes weakened later, the bacteria can reactivate and cause active TB. Fortunately, only about 10% of infected individuals develop active disease during their lifetime.
The hide-and-seek champion
When Mtb enters the lungs, the first cells it encounters are macrophages, the immune system’s professional “garbage collectors,” whose job is to engulf and destroy invading microbes. For most pathogens, this would be the end of the story. Mtb, however, has evolved remarkable ways to survive and even multiply inside these very cells that are supposed to kill it.
As infected macrophages accumulate, the immune system recruits many other immune cells to contain the infection within a structure called a granuloma, one of the defining features of TB. A granuloma is made up of different types of macrophages, including foamy macrophages and epithelioid cells, along with T cells, B cells, natural killer (NK) cells, and other immune cells. Think of it as a tiny prison built by the immune system to trap the bacteria.
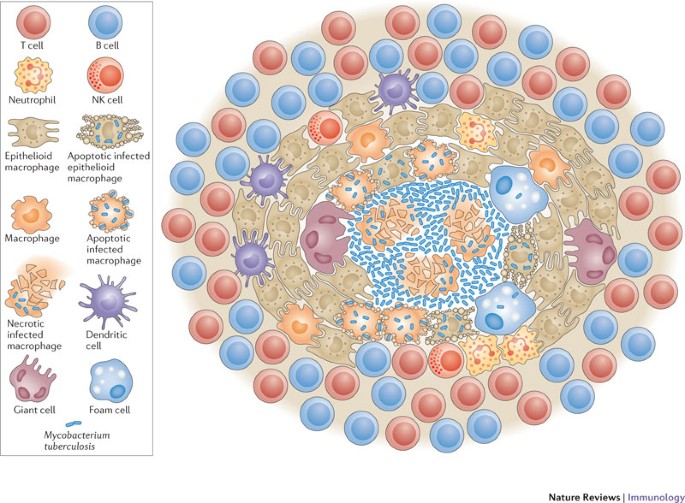
As the granuloma matures, conditions at its centre become increasingly hostile. Rather than being eliminated, Mtb adapts by entering a dormant state, allowing it to persist quietly within the body for years. If immunity weakens or the bacterial burden increases, the granuloma can break down into a cheese-like material called caseum, releasing the dormant bacteria and allowing the disease to reactivate and spread.
When the weapons stop working
As if surviving the immune system were not enough, Mtb also has another powerful survival strategy: resistance to antibiotics.
One of the most concerning forms is multidrug-resistant tuberculosis (MDR-TB), in which the bacterium becomes resistant to two of the most important first-line anti-TB drugs, isoniazid and rifampicin, making treatment far more difficult.
TB treatment is long, lasting anywhere from six months to two years depending on the type of infection and drug resistance. Side effects, treatment fatigue, and interruptions in medication can allow resistant bacteria to survive while susceptible ones are eliminated. Over time, these resistant strains of Mtb become dominant and continue spreading. What was once a treatable infection can therefore become a much greater challenge, not only for the patient but also for healthcare systems.
Fighting back
The thing about nature is that it lets only the fittest survive. Unfortunately for us, Mtb is very good at doing just that. Our response must be equally adaptive, beginning with early diagnosis while continuing to develop better tools to detect, treat, and prevent the disease.
Diagnosing TB involves several steps. Doctors first consider a person’s symptoms, medical history, and possible exposure to the disease. Tests such as the TB skin test or blood test can indicate whether someone has been infected. If TB is suspected, chest X-rays and laboratory analysis of sputum samples help determine whether the infection is active or inactive. Recently, WHO has recommended the wider use of rapid molecular diagnostic tests, which can detect TB and identify resistance to key antibiotics within a few hours.
Researchers are developing faster and more accurate diagnostic tools that can identify both the infecting strain of bacteria and drugs it is resistant to, helping doctors select effective treatments. Computer-aided chest X-ray screening is also making TB detection faster and more accessible. In recent years, newer all-oral regimens of antibiotics have increased success rates while reducing treatment duration, painful injections, and side effects. Meanwhile, multiple vaccine candidates are progressing through clinical trials, which may bring us closer to a world free of TB.
What can we do?
Fighting TB requires all of us to play our part.
If you are diagnosed with TB, it is important to take your medications as prescribed and complete the full course of treatment, even if you start feeling better. Stopping treatment early can allow the bacteria to survive and lead to antibiotic resistance.
Covering your mouth while coughing, ensuring good ventilation, and following your doctor’s advice can help prevent transmission.
Now, it is easy to think of TB in terms of bacteria, drugs, and statistics. Yet for millions of patients, TB is a deeply personal journey marked by uncertainty, lengthy treatment, and stigma. Stories shared by the survivors remind us that scientific advances alone are not enough; compassion, awareness, and community support are equally important in helping people recover.
Therefore, we must raise awareness and combat TB-related stigma. Early diagnosis, timely treatment, maintaining personal hygiene, consuming nutritious food and community support remain some of our strongest tools in the fight against this ancient pathogen.
Perhaps one of the most common questions people ask is why TB remains such a major problem in countries like India while it has become relatively uncommon in many Western nations. The answer is complex. It involves a combination of factors, including population density, healthcare access, delayed diagnosis, treatment interruptions, undernutrition, poverty, and the continued transmission of infection within communities. This is precisely why awareness remains just as important as advances in diagnostics, drugs, and vaccines.
TB is an ancient disease, but it is far from a disease of the past. Early diagnosis, timely treatment, continued research, and tackling stigma remain some of our strongest tools in ensuring that one day this remarkable survivor finally meets its match.
Niveditha A M is a first year PhD student in Infection Biology at NCBS, Bengaluru. Her research explores the complex interactions between Mycobacterium tuberculosis and the host immune system. She is also passionate about making infectious disease research accessible to the public through science communication.